
MCW Eye reVIEW Retina Quizzes

About Dennis P. Han, MD

Retina Quiz 1: Paracentral Scotomata and Blurred Vision



Retina Quiz 2: Esotropia and Amblyopia
VA Central, steady, maintained OD; Central, steady, unmaintained OS
Anterior segment exam was normal; there was no RAPD
Fundus exam showed a small gray inner retinal opacity in the perifoveal region of the right eye, and a gray, flat, macular lesion in the left eye. (see images to follow)
What life threatening condition(s) might this child develop in the future?


OCT (BIOPTIGEN) OD

OCT (BIOPTIGEN) OS

RETCAM FA OD

RETCAM FA OS

Retina Quiz 3: Choroidal Pigmentary Abnormalities
65 year old woman referred for choroidal pigmentary abnormalities RE
VA 20/100, pinhole to 20/70 RE, 20/25 LE
Right 3rd nerve palsy, corneal epithelial defects RE
History of a painful vesicular facial rash
Recent work-up for cerebral aneurysm negative
See fundus images to follow. Left fundus is normal.
What ocular condition does she have?





Patient History
- Prolonged, severe headaches, right-sided facial pain several weeks previously; evaluation for cerebral aneurysm negative
- Subsequently developed skin eruptions on right side of face in V1 distribution, subsequently developed 3rd nerve palsy, post-herpetic neuralgia, iridocyclitis, neurotrophic keratopathy RE: diagnosis of Trigeminal Herpes zoster made; managed with systemic acyclovir
- 7 weeks after skin eruptions, fundus examination noted to be normal OU; images seen here are a few months after that.
Tests
- Angiotensin converting enzyme: negative
- HLA A-29 negative
Retina Quiz 4: Difficulty Adapting to the Dark and Sparkles in Vision
63 year old woman with difficulty adapting to the dark and seeing sparkles in vision when going outside for the past year.
PMH: interstitial cystitis for 10 years
FH: No history of retinal degeneration or night blindness
BCVA OD 20/30; OS 20/20
Confrontation visual fields full OU
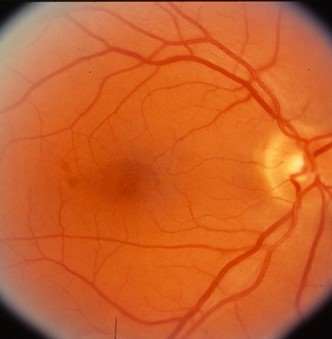
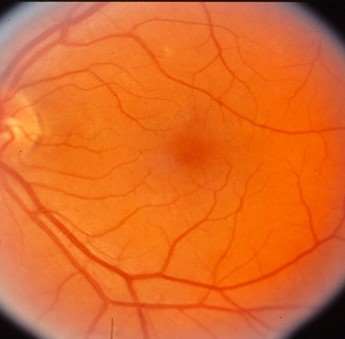
Fundus exam showed diffuse pigmentary abnormality OU
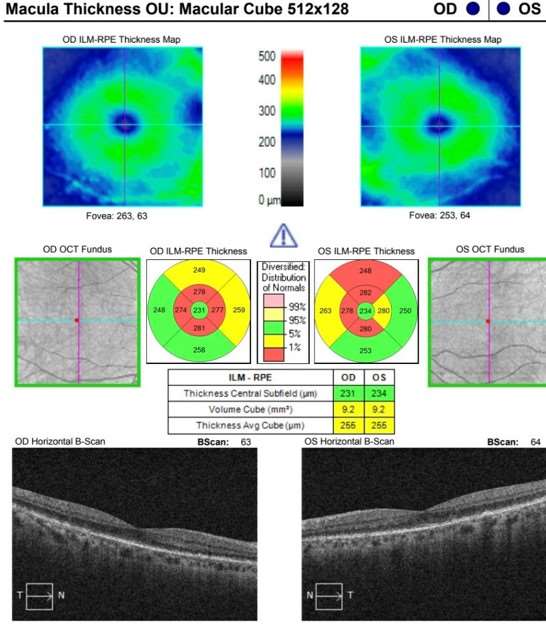
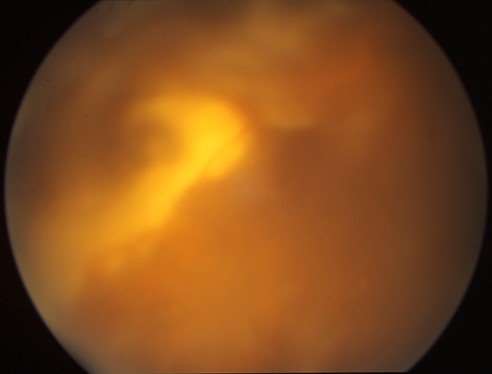
See color fundus photos, fluorescein angiogram, OCT scans to follow.
What condition should you suspect? What additional imaging modality might you obtain for improved follow-up?
DISC AND MACULA


FUNDUS PERIPHERY


OCT MACULA


Retina Quiz 5: Loss of Vision Upon Awakening
59 year old woman noted loss of vision OD upon awakening
History of fevers and chills beginning 10 days prior to presentation
Had dental procedures with amoxicillin prophylaxis 9 and 6 days prior to presentation (one day after onset of fevers)
VA OD 20/400, OS 20/25
See fundus images to follow; hemorrhages present OU.
What life threatening condition might she have?


The diagnosis for Case 5:
Subacute bacterial endocarditis with premacular hemorrhage OD--variants of the ”Roth spot” OU
- This patient had a history of mitral valve insufficiency. Upon hearing her history of fevers, and seeing her fundi, I drew three sets of blood cultures from her on the spot. All three were positive for S. viridans, supportive of a diagnosis of subacute bacterial endocarditis. She did well after a course of IV penicillin and gentamicin. (see slides to follow).
- This woman came to me about 15 years later (around 2015), not as a patient, but bringing a friend for an eye exam, and thanked us for saving her life. I ran into her just a few feet from where I drew her cultures, on the 2nd floor at the EI.
- The lesson here is that the “white centered hemorrhages” associated with SBE can vary in appearance. Here, in the right eye, the hemorrhagic component predominated over the white areas. In the left eye the “white center” had only a very small hemorrhage.
- We thought the case was unusual enough that Dr. Judy Kim and I published it. The article accompanies this file. See this patient’s course and other examples of Roth spots to follow.
Supporting Study:
Premacular Hemorrhage as a Sign of Subacute Bacterial Endocarditis
Diagnosis Follow Up:
Two and a half Months later after course of intravenous PCN for streptococcus viridans subacute bacterial endocarditis
VA OD 20/25 OS 20/20
Retina Quiz 6: Juvenile X-Linked Retinoschisis
Genetic counseling
Gene therapy trials ongoing
Laser treatment indicated only to demarcate existing progressive subclinical RD with outer layer holes or full-thickness breaks
Scleral buckling or vitrectomy for clinical RD
Vitrectomy for recurrent or nonclearing VH; vitreous hemorrhages are presumed to be from perfused vessels remaining in the elevated schitic layer of the retina that have traction on them. If they break and bleed, and become completely divided, they likely will not bleed again. In recurrent cases of VH, some advocate removing the inner retinal layer(cauterizing and dividing bridging vessels) so that further traction on the vessels cannot occur. --DPH
ALL of these laser/surgical interventions are rarely needed.


Macular SD-OCT showing schitic cavities in XLRS:


Right Eye Left Eye
Retina Quiz 7: Floaters and History of High Myopia
This 46 yr old woman complained of floaters OD for 6-7 months. Past ocular history was significant for high myopia.
Visual acuity was 20/20 OU. Anterior chamber was quiet. There were 1+ - 2+ pigmented cells in the vitreous OD. A posterior vitreous separation and peripheral operculated hole were presented OD.
No FHx of ocular lesions, eye or brain tumors, or tumors elsewhere.
What’s in your differential diagnosis?








Retina Quiz 8: Red, Painful Eye and Blurry Vision
40 y/o woman noted a red, painful right eye 10 days previously and blurry vision 2 days previously. Immigrated from Mexico 3 yrs previously. ROS negative.
VA OD 3/200; OS 20/25
Superior VF defect OD, normal OS
Slit lamp exam
OD: 1+ diffuse bulbar conj hyperemia, mild KP, 3+ AC cell, lens clear, 2+ anterior vitreous cell
OS: normal
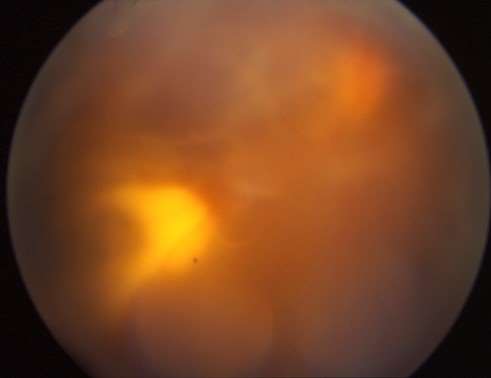
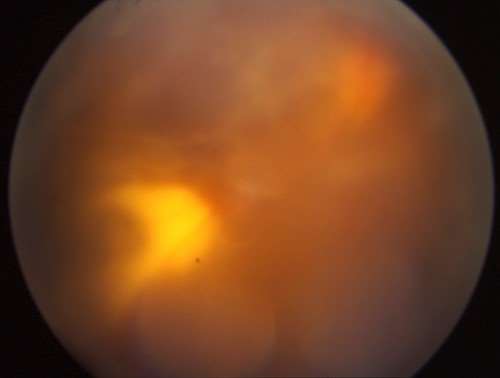
Fundi: OD—see slides; OS—normal


The diagnosis for Case 8:
- Toxoplasmic retinochoroiditis.
- Important Diagnostic Clue: This is primarily a retinal opacity that is adjacent to a pigmented chorioretinal scar. (This finding is most noticeable on the 2nd image of the fundus.) Note: Viral retinitis (ARN) is also known to recur at margins of previous involvement, but is usually more peripheral in location.
- This patient underwent oral antitoxoplasmic therapy but was eventually lost to follow-up. A set of stereo photographs taken after treatment initiation shows what may be partial regression over a number of weeks with persistent vitreous opacities. (Try converging your eyes until you see three images and concentrate on fusing the middle one.)

Questions about our Retina Quizzes?
Email us at Ophthalmology@mcw.edu.