
Case Study 19 - CC: Wandering Eye and Double Vision
Original Authors: Rebecca Mastey, MD, Heather Stiff, MD
HPI:
8 year old female brought in by mother for evaluation of wandering eye and double vision. She was noted to have eye misalignment at age 1 and age 2 but exams were limited at that time. The patient had not followed with ophthalmology since then. Recently, the right eye has been wandering more frequently and has been noticed by teachers and students at school. She also gets double vision when she looks up and has adapted a slight chin up posture.
Past Ocular History:
Intermittent exotropia noted at age 1 and 2
Ocular Medications:
None
Past Medical History:
None
Surgical History:
None
Past Family Ocular History:
None
Social History:
Lives with parents and older sister. Normal growth and development for age.
Medications:
Allegra
Allergies:
NKDA, seasonal allergies
ROS:
Denied headache, denied recent illness
Ocular Exam
Visual Acuity (cc):
OD: 20/50 +1
OS: 20/50 +3
Pupils:
OD: Dark 8, Light 6, Round, Risk, No APD
OS: Dark 8, Light 6, Round, Risk, No APD
Extraocular Movements:
OD: -3 to supraduction, otherwise full
OS: Full
Confrontational Visual Fields:
OD: Full
OS: Full
Slit Lamp Exam:
| RIGHT EYE | LEFT EYE | |
| External | Normal |
Normal |
| Lids and Lashes | Normal | Normal |
| Conjunctiva/Sclera | White and quiet | White and quiet |
| Cornea | Clear |
Clear |
| Anterior Chamber | Deep and quiet | Deep and quiet |
| Iris | Normal | Normal |
| Lens | Clear | Clear |
| Anterior Vitreous | Normal | Normal |
| RIGHT EYE | LEFT EYE | |
| Disc | Normal | Normal |
| C/D Ratio | 0.2 | 0.2 |
| Macula | Normal | Normal |
| Vessels | Normal | Normal |
| Periphery |
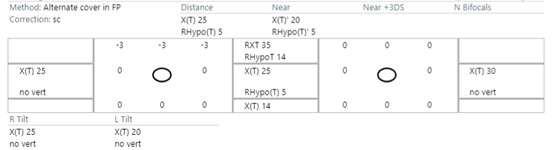
Imaging/additional tests:
Sensorimotor exam:
- Stereo: Animals 3/3, Circles 8/9
- Abnormal head position (AHP): 5-10 degree chin up
Case Studies
-
Ophthalmic Case Study 1
Acute right eye pain -
Ophthalmic Case Study 10
Blurry vision in the left eye for 2 weeks -
Ophthalmic Case Study 2
Red, itchy eyes -
Ophthalmic Case Study 11
Acute pain and burning in L eye -
Ophthalmic Case Study 3
Acute left eye pain and blurry vision -
Ophthalmic Case Study 12
Blurry vision in both eyes and headaches -
Ophthalmic Case Study 4
Left eye pain and fuzzy vision 2 days after eye surgery -
Ophthalmic Case Study 13
"Cannot see well" from left eye -
Ophthalmic Case Study 5
Girl rubbing her R eye after trauma -
Ophthalmic Case Study 14
Blurry vision in both eyes -
Ophthalmic Case Study 6
Red eye and pain on the left -
Ophthalmic Case Study 15
Eye irritation and dryness -
Ophthalmic Case Study 7
Vision loss L eye -
Ophthalmic Case Study 16
2 brief episodes of vision loss in the R eye -
Ophthalmic Case Study 8
Crossed eyes -
Ophthalmic Case Study 17
Routine eye exam -
Ophthalmic Case Study 9
White pupils -
Ophthalmic Case Study 18
Case Study 18 - CC: 8-year-old boy presents with difficulty seeing whiteboard at school -
Ophthalmic Case Study 20
Red eyelid lesion in an infant -
Ophthalmic Case Study 21
Female patient with optic nerve abnormality